

Patella tendinitis
This condition is also called jumper’s knee. 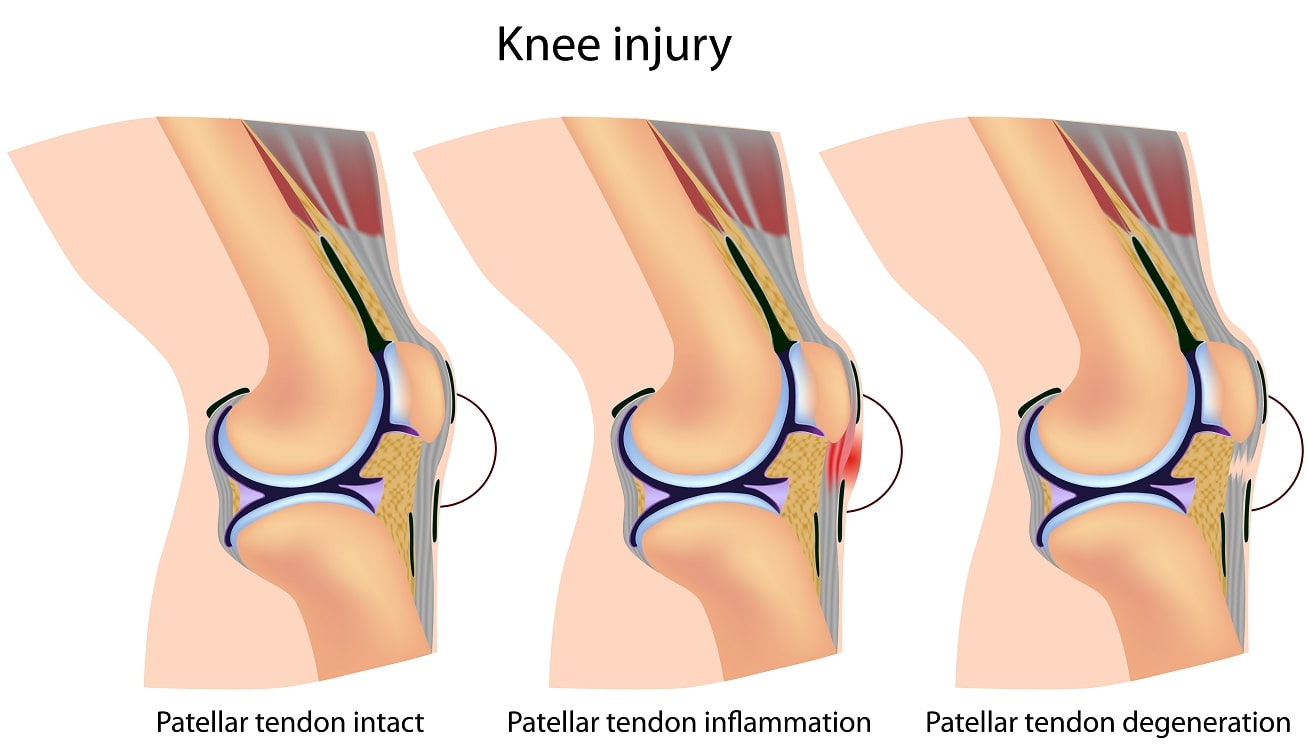
It is anterior knee pain with is associated with activity. There is focal patella tendon tenderness at the lower border of the knee cap. In the initial phase there is pain following activity and later there is pain with activity and with prolonged knee flexion. The mechanism responsible for symptoms is repetitive eccentric contraction of the extensor apparatus. It is often associated with poor quadriceps and hamstring flexibility. When checking the tendon under the microscope there are degenerative rather than inflammatory changes and micro-tears are commonly seen. Jumping sports in particular Volleyball are risk factors. RICE (rest, ice, ©- strapping, eccentric exercises are the mainstay of treatment. Surgical treatment is indicated in severe cases (persistent pain with or without activity, deterioration if performance). The degenerative tendon tissue is removed and the tendon repaired. Return to sports is achieved by 80% of patients but there may be activity related pain for up to 6 months after surgery.
Quadriceps tendinitis
Similar to jumper’s knee repetitive contractions of the extensor mechanism can cause pain at the proximal aspect of the knee cap. Micro-tears are seen at the bone-tendon interface. 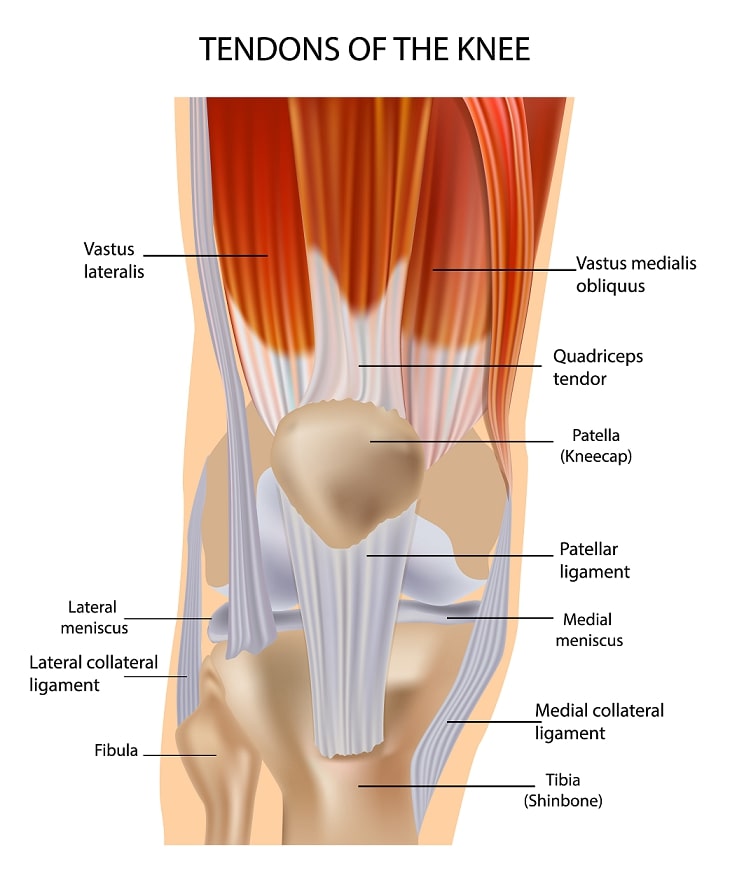 Pain is localized at the insertion of the quadriceps tendon into the patella. Treatment follows the guidelines for Jumper’s knee. Surgery is very rarely indicated. Cortisone injections are strictly contraindicated as they can cause tendon ruptures.
Pain is localized at the insertion of the quadriceps tendon into the patella. Treatment follows the guidelines for Jumper’s knee. Surgery is very rarely indicated. Cortisone injections are strictly contraindicated as they can cause tendon ruptures.
Semimembranosus Tendinitis
This is a condition which is common in male endurance athletes often in their thirties. There is pain in the posteromedial knee which may radiate into the thigh or calf .  On physical examination there is tenderness on the tibial insertion and passive deep knee flexion or internal rotation of the knee in flexion may increase pain and symptoms. The Jumper’s knee treatment is the mainstay but a cortisone injection can be a very helpful adjunctive measure if there is limited improvement with physical therapy.
On physical examination there is tenderness on the tibial insertion and passive deep knee flexion or internal rotation of the knee in flexion may increase pain and symptoms. The Jumper’s knee treatment is the mainstay but a cortisone injection can be a very helpful adjunctive measure if there is limited improvement with physical therapy.
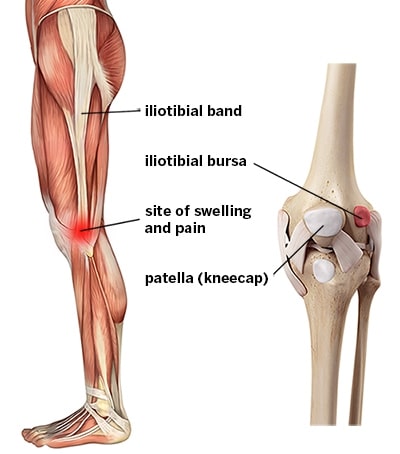 Iliotibial Band Friction Syndrome
Iliotibial Band Friction Syndrome
The iliotibial band (ITP) is a structure originating in the hip and is the continuation of the tensor fascia lata. It inserts into the tibia. Pain is predominantly located over the lateral femoral condyle and is often worse with changes in running terrain, sloped surfaces and increase in mileage. Malalignment of the knee (varus) or the foot (flatfoot) are risk factors. “Joint” crepitus, reduced hip and knee motion, weakness of hip abduction and pain with a single leg squat are physical signs. The Ober test (lateral position with the knee flexed to 90 degrees and bringing the hip from flexion and abduction into extension and adduction) reproduces symptoms and is positive if there is pain, tightness or clicking over the ITB. Non-operative treatment consisting of rest, ice, anti-inflammatory medication, cortisone injections and training modifications are the primary treatment options. Failed non-operative treatment is an indication for surgery. Elliptical excision of the ITB or a Z-Plasty of the ITB are surgical options.